
Snoring, Mouth Breathing, and Sleep Issues in Children – Gentle Therapy That Supports Focus, Growth, and Restful Nights
Helping Children Breathe Better, Sleep Deeper, and Thrive Naturally
National SleepFoundation.org:
“Doctors are starting to realize the importance of treating sleep problems and the impact this can have on both ADHD symptoms and quality of life for ADHD patients and their families.
An estimated 25 to 50% of people with ADHD experience sleep problems, ranging from insomnia to secondary sleep conditions.”
If your child snores, breathes through their mouth, or struggles with focus and fatigue, the problem could be poor sleep—and we treat the root cause.
Children & Adults Behave Differently When Sleep Deprived:
"Adults become sluggish, where children overcompensate and speed up.
Children may also become moody, emotionally explosive, aggressive, inattentive, hyperactive, impulsive and display oppositional behaviors."11,13,14,15
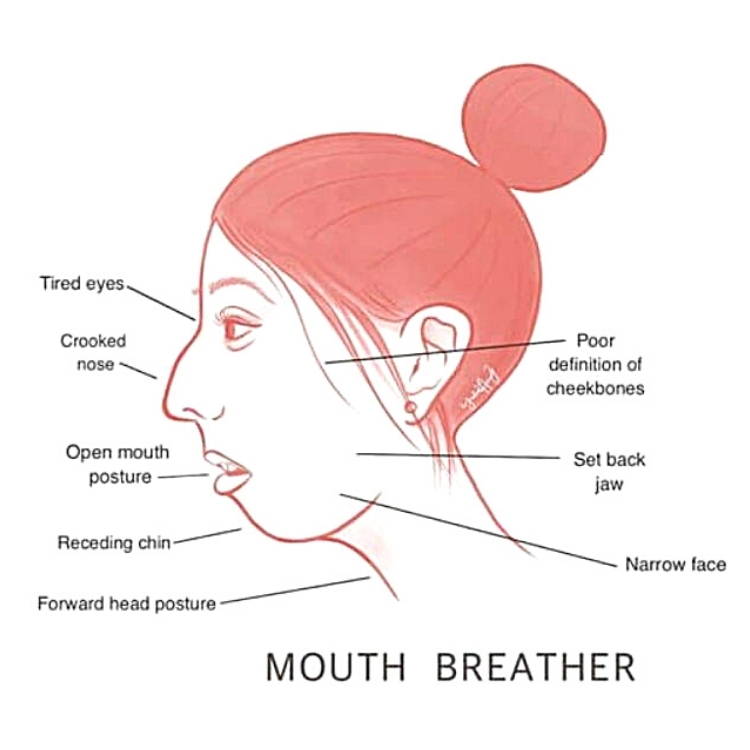
Is Your Child Starting to Display Any Of These Symptoms?
Causes Long Face Syndrome11,16,19,23
Crooked Teeth
Narrow Jaw and Face
Poorly Defined Cheekbones
Tired Eyes
Jaw Set Back
Smaller Airway
Underdeveloped Nasal Airway
Poor Posture

Brain Fog11
Decreased Productivity8,9,10,11,23
Poorer Academics: Performing Poorly at School11
Poorer Quality of Life8,9,10
Increased Stress24
Decreasing Health
Tired8,9,10,11,23
Reduced Growth Hormone Production: May not be growing as fast as their peers. Takes a while to heal.31,32,33


Sleep Apnea: Breathing Stops While Asleep for a Varying Length of Time
Dry Mouth, Sore Throat, Headaches, Trouble Paying Attention, & Irritability12
Memory Loss: Sleep helps to consolidate memories12
Mental Confusion12
Weakened Immune System: Reduced number of T-cells12
Depression6
Fatigue12
High Blood Sugar Levels3
Deprives Body of Needed Oxygen Levels12
Acid Reflux12
Asthma5
What is Orofacial Myofunctional Therapy Capable Of?
At Oral-Facial Advantage, we guide your child's growth towards a more balanced oral-facial foundation. Aiding to prevent, or soothe the many disorders you see through-out this website.
Reflexive vs. Conscious
We chew, swallow, breathe, and rest our mouths as an un-trained reflexive habit.
The Oral-Facial Advantage Program is a personalized straightforward set of exercises, scientifically designed to build new beneficial long-term muscle-memories.
At What Age Can My Child Begin Oral-Facial Muscle Therapy?
The younger the child the more flexible their physiology and behavior.
Mature 3 to 4 year old mouth breathers can learn nasal breathing.
Mentally prepared 5 year old's can begin the Oral Habit Elimination Program.
7 to 8+ year old's can start their Oral-Facial Advantage Program.
Who is Eligible for a Free Consult?
Everyone.
All ages can come in for a free consult.
It is a great opportunity for your questions to be answered, and for the Orofacial Myologist to assess your child's readiness for the program.
Book a Free In-Person Consultation Today
Benefits of Orofacial Myofunctional Therapy
Soothes or relieves headaches
Can help reduce snoring & apnea
May reverse some ADHD symptoms
Opens upper airways
Can prevent long face syndrome
Alleviates facial pain
Improves posture & core muscle stability
Increases jaw range of motion
Facial symmetry: Tones facial muscles & tissues
Improves focus, memory, productivity
Lowers harmful stress hormones
Relieves digestive discomfort
Eliminates habits involving the mouth
Much more
What is Orofacial Myofunctional Therapy?
The mouth, head, and neck are a complex weave of muscles, tissues, joints, bones, blood vessels, and nerves that all need to work together for a smooth, discomfort free daily function.
Currently, we are born and grow with little direction and training in this area of our bodies. We eat the way we eat, we chew on the side that is most comfortable, we swallow whichever way gets the food down, our tongues rest wherever they rest, we breathe the easier way, and we have repetitive habits that soothe our stress that can involve our faces and mouths.
All of these reflexive habits can create abnormalities in your child's oral and facial structures, and since they have been doing them throughout their youthful growth, their bones and muscles have molded around these untrained habits, potentially creating ingrained disorders in their later years.
Orofacial Myofunctional Therapists specialize and only focus on the muscles and tissues throughout the tongue, jaw, face, head, and neck. Weekly exercises are given that either tone or relax these muscles and tissues aligning them to your child's center. Working from their foundation up. Progressively resetting years of habits. Most children will complete the program within the year and yet their new symmetry could last their lifetime.
A Stanford University Systematic Review revealed the lasting beneficial effects of Orofacial Myofunctional Therapy in a wide cohort:
“Current literature demonstrates that orofacial myofunctional therapy decreases apnea-hypopnea index by approximately 50% in adults and 62% in children. Improvements to snoring and daytime sleepiness. Shown effective in children and adults of all ages studied thus far; youngest patient 3 yrs old to 60 yrs old. Therapy has an important role in preventing relapse.”48
1Key, Josephine. “‘The core’: understanding it, and retraining its dysfunction.” Journal of bodywork and movement therapies 17, no. 4 (2013): 541-559.
2Gunduz C, et al "Obstructive sleep apnea independently predicts lipid levels: Data from the European Sleep Apnea Database" Respirology 2018; DOI: 10.1111/resp.13372.
3Jimmy Doumit, Bharati Prasad. "Sleep Apnea in Type 2 Diabetes" Diabetes Spectrum 2016 Feb; 29(1): 14-19.
4Omar A. Mesarwi, Rohit Loomba, Aul Malhotra. "Obstructive Sleep Apnea, Hypoxia, and Nonalcoholic Fatty Liver Disease" ATS Journals 2018 Nov; V199, I7.
5Bharati Prasad, Sharmilee M. Nyenhuis, Ikuyo Imayama. "Asthma and Obstructive Sleep Apnea Overlap: What has the evidence taught us?" ATS Journals 2019 Dec;V201, I11.
6Ejaz, Shakir M et al. “Obstructive sleep apnea and depression: a review.” Innovations in clinical neuroscience vol. 8,8 (2011): 17-25.
7Djupesland PG, Chatkin JM, Qian W, Haight JS. Nitric oxide in the nasal airway: a new dimension in otorhinolaryngology. Am J Otolaryngol.2001 Jan; 22(1): 19-32.
8Lunn M, Craig T. Rhinitis and sleep. Sleep Med Rev. 2011 Oct;15(5):293-9
9Muliol J, Maurer M, Bousquet J. Sleep and allergic rhinitis. Journal Investigation Allergol Clinical Immunology. 2008;18(6):415-9.
10Ohki M, Usui N, Kanazawa H, Hara I, Kawano K. Relationship between oral breathing and nasal obstruction in patients with obstructive sleep apnoea. Acta Otolaryngol Suppl. 1996;523:228-30.
11Jefferson Y. Mouth breathing: adverse effects on facial growth, health, academics and behaviour. General dentist. 2010 Jan- Feb; 58 (1): 18-25.
12Fitzpatrick MF, McLean H, Urton AM, Tan A, O’Donnell D, Driver HS. Effect of nasal or oral breathing route on upper airway resistance during sleep. Eur Respir J. 2003 Nov;22(5):827-32.
13“ADHD and Sleep.” ADHD & Sleep Problems-National Sleep Foundation. National Sleep Foundation, 2017. Web. 11 Feb.2017. https://sleepfoundation.org/sleep-disorders-problems/adhd-and-sleep.
14Shur-Fen Gau S. Prevalence of sleep problems and their association with inattention/hyperactivity among children aged 6-15 in Taiwan.J Sleep Res. 2006 Dec;15(4):403-14.
15Borres MP. Allergic rhinitis: more than just a stuffy nose. Acta Paediatrica. 2009 Jul;98(7):1088-92)
16Pereira F, Motonaga S, Faria P, Matsumoto M, Trawitzki L, Lima S, Lima W. Myofunctional and Cephalometric Evaluation of Mouth Breathers. Brazilian Journal of Otorhinolaryngology. 2001. 67 (1): 43-49.
17Garliner D. Myofunctional Therapy. Philadelphia: Saunders, 1976. Print.(10-12)
18John E. Hall, Arthur C Guyton. Tongue posture and swallowing. Guyton and Hall textbook of medical physiology, 12th edition. 2010; 763-765.
19Paskay L. OMD Orofacial Myofunctional Disorders: Assessment, prevention and treatment. JAOS. 2012 march-april; 34-40.
20Okuro RT, Morcillo AM, Ribeiro MÂ, Sakano E, Conti PB, Ribeiro JD. Mouth breathing and forward head posture: effects on respiratory biomechanics and exercise capacity in children. J Bras Pneumol.2011 Jul-Aug; 37(4):471-9.
21Damaging Effects of Forward Head Posture.(2015, January 22). Retrieved from http://www.denvertechchiro.com/files/fhp_revised.pdf
22Svensson S, Olin AC, Hellgren J. Increased net water loss by oral compared to nasal expiration in healthy subjects. Rhinology. 2006 Mar;44(1):74-7. PMID: 16550955.
23Surtel A, Klepacz R, Wysokińska-Miszczuk J. Wpływ toru oddechowego na jamę ustną [The influence of breathing mode on the oral cavity]. Pol Merkur Lekarski. 2015 Dec;39(234):405-7. Polish. PMID: 26802697.
24Steffen, Patrick R et al. “The Impact of Resonance Frequency Breathing on Measures of Heart Rate Variability, Blood Pressure, and Mood.” Frontiers in public health vol. 5 222. 25 Aug. 2017, doi:10.3389/fpubh.2017.00222
25Tongue-tie (ankyloglossia). American Academy of Otolaryngology-Head and Neck Surgery. http://www.entnet.org/content/tongue-tie-ankyloglossia. Accessed Feb. 13, 2018.
26Isaacson GC. Ankyloglossia (tongue-tie) in infants and children. https://www.uptodate.com/contents/search. Accessed Feb. 14, 2018.
27Chinnadurai S, et al. Treatment of ankyloglossia for reasons other than breastfeeding: A systemic review. Pediatrics. 2015;135:e1467.
28Baker AR, et al. Surgical treatment of ankyloglossia. Operative Techniques in Otolaryngology. 2015;26:28.
29Walsh J, et al. Diagnosis and treatment of ankyloglossia in newborns and infants. JAMA Otolaryngology-Head and Neck Surgery. 2017;143:1032.
30O'Shea JE, et al. Frenotomy for tongue-tie in newborn infants. Cochrane Database of Systemic Reviews. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD011065.pub2/abstract. Accessed Feb. 14, 2018.
31Davidson, J R et al. “Growth hormone and cortisol secretion in relation to sleep and wakefulness.” Journal of psychiatry & neuroscience : JPN vol. 16,2 (1991): 96-102.
32Takahashi, Y et al. “Growth hormone secretion during sleep.” The Journal of clinical investigation vol. 47,9 (1968): 2079-90. doi:10.1172/JCI105893
33Honda, Y et al. “Growth hormone secretion during nocturnal sleep in normal subjects.” The Journal of clinical endocrinology and metabolism vol. 29,1 (1969): 20-9. doi:10.1210/jcem-29-1-20
34Morabito G, et al. (2014). Functional aerophagia in children: A frequent, atypical disorder. DOI:10.1159/000362441
35Timmons, Beverly H., and Ronald Ley. “Behavioral and Psychological Approaches to Breathing.
35https://news.stanford.edu/2020/07/21/toll-shrinking-jaws-human-health/

By Jul 15, 2026

By Jan 04, 2026
By Oct 12, 2025

By Oct 01, 2025

By Aug 10, 2025